Arthur J. Siegel, Medical Director at MGH Internal Medicine Associates, Belmont, MA, USA tells us how low-dose aspirin can support primary prevention of marathon-related cardiac arrest in middle-aged men with coronary atherosclerosis
While habitual endurance exercise such as training for a marathon is quintessentially cardioprotective, running the 26.2 mile race transiently increases the risk for cardiac arrest and sudden cardiac death. (1) Male gender and the marathon were identified as significant and independent risk factors for race-associated cardiac arrest in a ten-year registry of United States road races beginning in the year 2000, in which events increased significantly in frequency during the study. (2)
Fatalities occurred mainly in middle-aged men with coronary atherosclerosis, as shown in a concurrent retrospective report. An explanation for this counterintuitive paradox may emerge by connecting the dots from such premature race-related cardiac mortality to observational studies in middle-aged male Boston marathon physician-runners. The latter shows that these asymptomatic subjects cross the finish line with inflammatory biomarkers showing the same ‘cytokine storm’ characteristic of patients who are undergoing an acute myocardial infarction. In the absence of contraindications, pre-race aspirin use is prudent for runners with subclinical coronary atherosclerosis to attenuate the transiently elevated risk for cardiac arrest during the race. This measure additionally provides those at risk with the benefit of having on board the only substance the American Heart Association recommended for pre-hospital administration in acute coronary syndromes.
Novel pathogenic considerations
An explanation for this counterintuitive paradox may emerge from observation, as a concurrent retrospective report shows. (3) Studies in asymptomatic middle-aged male Boston marathon physician-runners were carried out over sequential races. Post-race inflammatory biomarkers demonstrated the same ‘cytokine storm’ characteristic of patients during an acute myocardial infarction. Activation of atherothrombosis also occurred, including in vivo activation of platelets. (4,5)
Inflammation due to exertional rhabdomyolysis after ‘hitting the wall’ resulted in a perfect storm for triggering acute coronary thrombosis, as has been documented in Boston marathon runners after races. (6,7) Analogous to the pro-atherogenic inflammatory response reported after SARS-CoV-2 infection in human coronary vessels, (8) this sequence validates the hypothesis that skeletal muscle injury can damage the heart as advanced in the first study of Boston marathon runners after the inaugural race in 1897. (9)
Attenuating the transiently increased race-related risk
The increasing frequency of cardiac arrests in middle-aged men during marathons since 2000 warrants an expedited search for an action plan to mitigate such premature cardiovascular morbidity and mortality. Low-dose aspirin use has been recommended as a candidate for this purpose, connecting the cardiac arrests in middle-aged male runners with subclinical coronary atherosclerosis to the post-race findings in asymptomatic same-aged physician-runners.
It was based initially on evidence that low-dose aspirin use resulted in a 40% reduction in first heart attacks in healthy middle-aged male physicians in the final report on aspirin in the Physicians Health Study, a randomized controlled primary prevention trial. (10)
Another randomized controlled trial showed a 30% reduction in major acute cardiac events in persons at intermediate baseline cardiac risk with the addition of aspirin in the polypill investigations. (11) However, such a ‘gold standard’ trial, specifically in runners, lacks feasibility due to the low incidence of index events.
Low-dose aspirin use for enhanced primary prevention
The anti-inflammatory and anti-thrombotic properties of aspirin position it for enhanced primary prevention of race-related acute cardiac events, similar to the recommendation for using low-dose colchicine for its anti-inflammatory effects in patients with acute myocardial infarction. (12) This measure additionally provides an at-risk runner with the benefit of having an agent on board pre-emptively with a class 1A recommendation for pre-hospital administration in acute coronary syndromes.
Improved risk stratification to guide low-dose aspirin use
C-reactive protein levels and coronary artery CT calcium scoring (CACS) are candidates to assist middle-aged male marathon runners regarding informed decisions on aspirin. (13, 14) While levels of the former peak after races and are variably elevated during training, CACS reliably assesses subclinical coronary atherosclerosis, thereby predicting risk for major acute cardiovascular events, including sudden cardiac death. (15, 16) Such testing is recommended for novice and experienced runners, as the latter may have elevated scores due to high levels of participation in endurance exercise, even if in the lowest quartile of risk by traditional calculators. (17, 18)
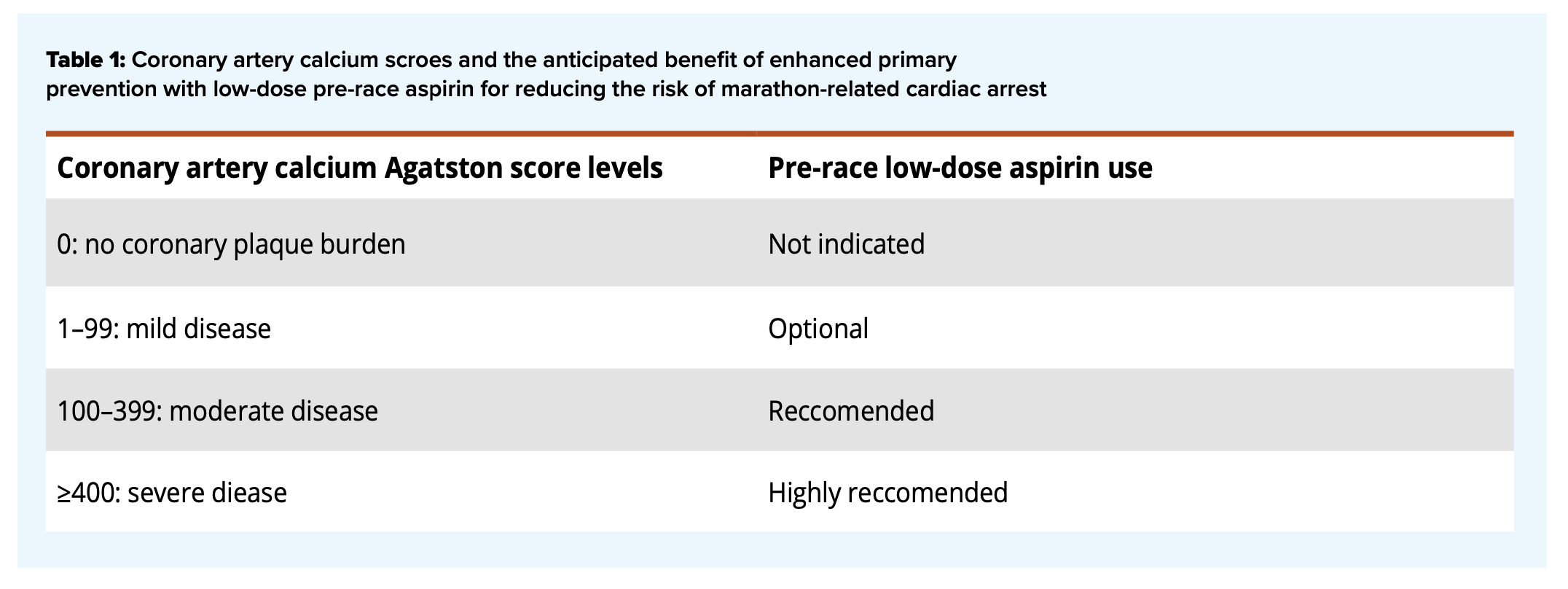
The anticipated benefit of low-dose aspirin use varies according to CACS results, as shown in Table 1. In the absence of clinical contraindications, scores over 100 Agatston units qualify for aspirin use based on increasing risk for acute cardiac events, including sudden cardiac death. (19, 20) Enhance primary prevention with aspirin has similarly been recommended for individuals with elevated lipoprotein(a). (21)
Low-dose aspirin use is prudent to minimize the transiently elevated race-related risk for cardiac arrest in middle-aged male marathon runners with subclinical coronary atherosclerosis. (22)
Dr Siegel is an Associate Professor of Medicine at Harvard Medical School, Boston, MA, USA, and a Fellow of the American College of Physicians.

This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International.