Professor Adèle Ehongo discusses her work in context of the ophthalmology department
The ophthalmology department of the Erasme Hospital provides clinical and surgical activity. Surgery is mainly performed on an outpatient basis.
This is a reference center that draws patients from different backgrounds and treats all preventive and therapeutic aspects of ocular pathology, including myopia and glaucoma.
Recent progress in understanding the onset of myopia has resulted in a change in its early-stage management, which aims to reduce its complications, which are responsible for visual disability. Among these complications, visual field deficits stand out because they impose themselves on glaucoma and, therefore, constitute the meeting point of the two conditions.
The management of glaucoma in our department is done within a team that is structured around three main axes centered on the patient. Several technicians carry out the acquisition of the examinations essential for the baseline assessment or the progression analysis of the disease. Doctors in training in ophthalmology (who change every six months) constitute the second axis of this sector. Finally, a glaucoma specialist (me) coordinates the whole. It is a team that, although small, is dynamic and called to grow.
Glaucoma assessment
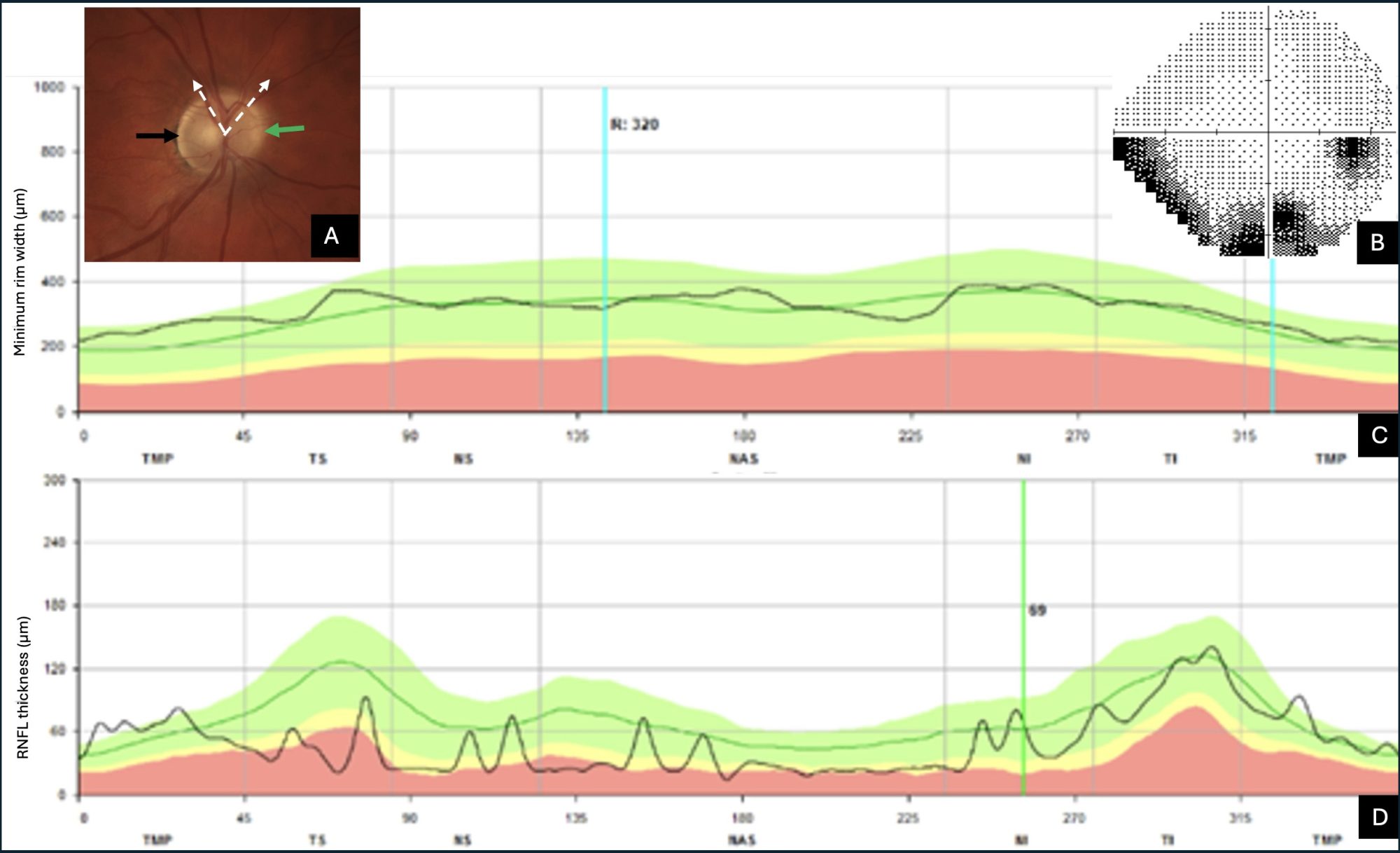
Glaucoma assessment includes two components. On the one hand, the functional aspect is explored essentially by the visual field (which is the part of the space perceived when we look straight ahead) testing. On the other hand, the structural analysis addresses the optic nerve and the macula. The exploration of the structure is done using Optical Coherence Tomography (OCT), which provides a quantified analysis of the parameters, thus completing the purely qualitative information provided by the photos. OCT has become an essential tool in the diagnosis of eye pathologies. In glaucoma clinics, it provides information ready to use by classifying it in terms of normal, borderline or pathological.
Interestingly, the capabilities of this tool are still underused, especially when we only consider the results provided in all sets. Thus, a few simple gestures not routinely performed during the interpretation phase and which do not prolong it make it possible to identify certain pathologies which, at first glance, can mimic glaucoma. This simple precaution avoids costly and anxiety-provoking investigations for the patient.
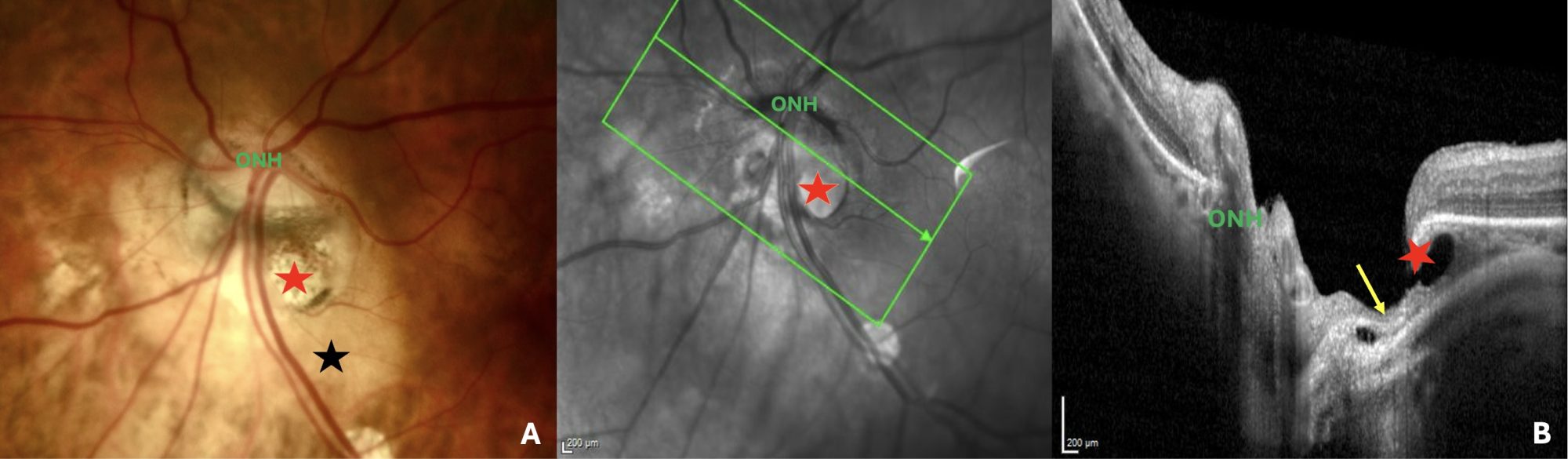
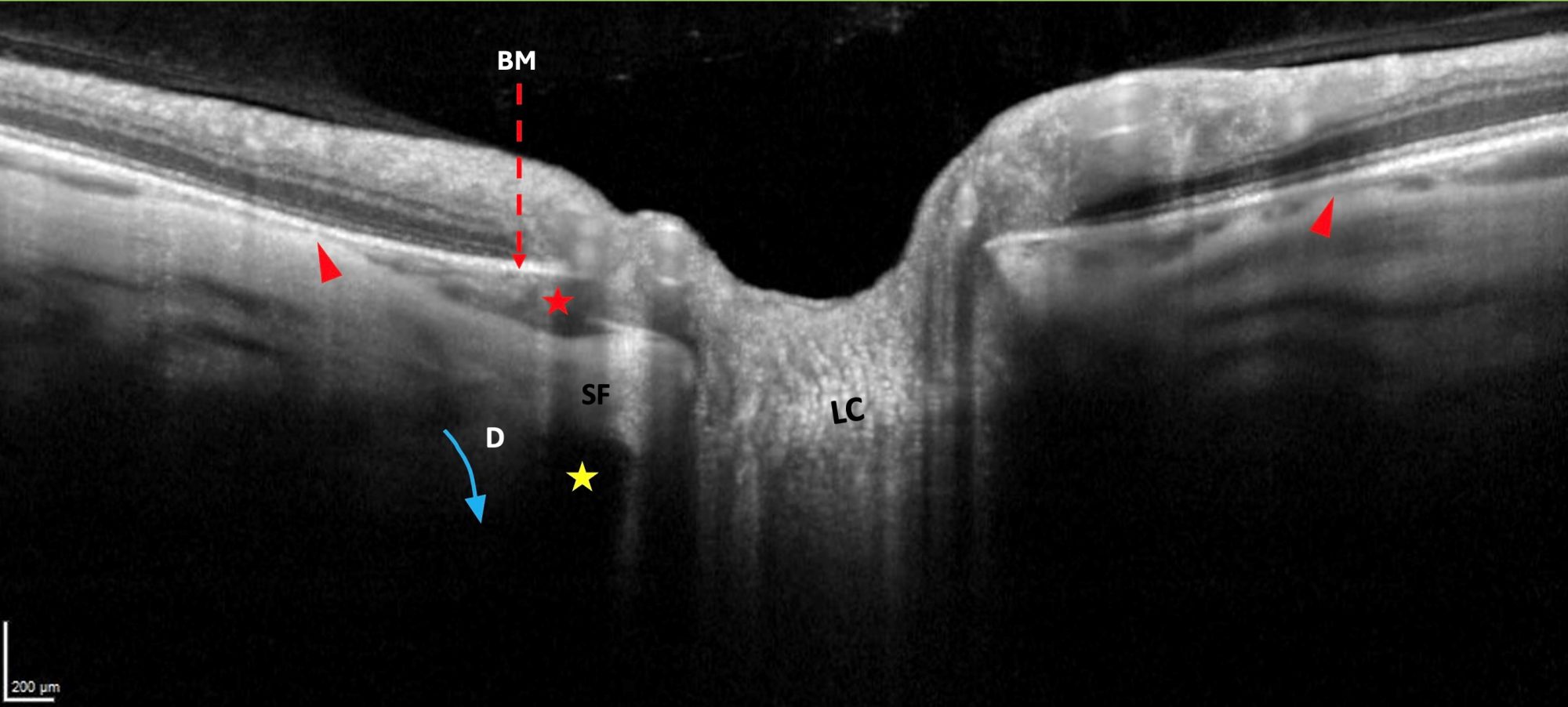
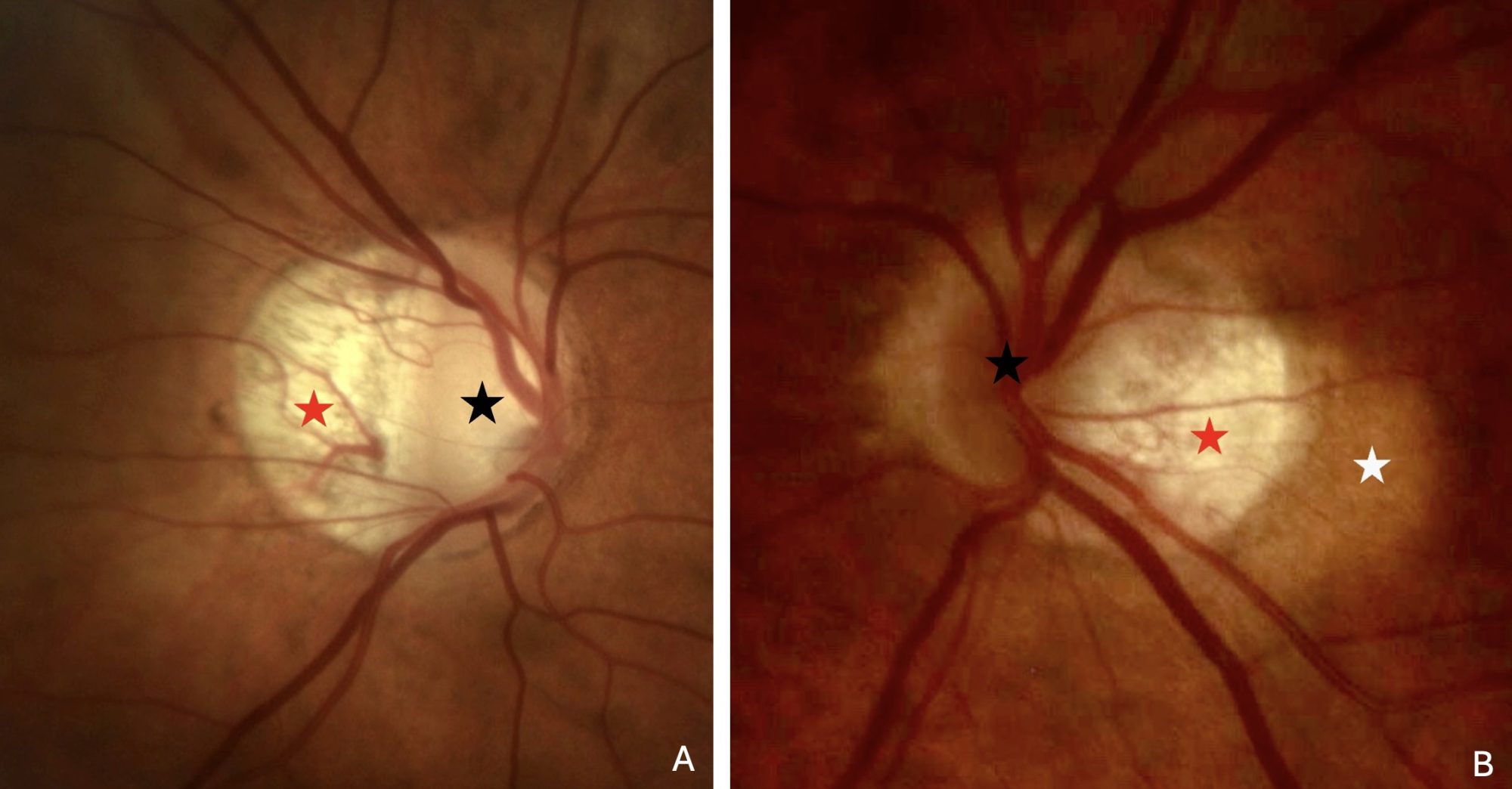
This is how five years ago, on my initiative, our study on peripapillary complications of myopia was launched in our team, giving very interesting results on peripapillary intrachoroidal cavitation and emphasizing the importance of the clinician not relying solely on ready-made results in his daily practice.
My interest remains in glaucoma masquerades, including myopic complications.